Dialysis
It is a process by which an attempt is made to maintain the functions of kidney in the absence of normal renal function.
Complications due to Dialysis
1. Haemorrhage - They pump a drug called Heparin to prevent clotting
of blood in the tubes, during Dialysis.
2. Hypotension - Low BP, as salt (sodium) is removed from the body.
It is very essential to maintain normal BP, else results in low BP.
3. Cardiac Ischaemia - Continuous Dialysis sometimes results in blockage
or compression of major blood vessels.
4. Cramps - This occurs almost to everyone unless they follow certain
rules before Dialysis (described in the last section of HD). The other
reason is, if excess fluid removed during Dialysis.
5. Nausea and Vomiting Whenever there is low BP, the patient tends
to have nausea and in severe cases, vomiting.
6. Seizures (fits) - Very rare cases.
7. Hypoventilation Decreased air exchange in the lungs.
Types of Dialysis
1. Intermittent Peritoneal Dialysis (IPD)
2. Continuous Ambulatory Peritoneal Dialysis (CAPD)
3. HaemoDialysis (HD)
Intermittent Peritoneal Dialysis
This is actually removing excess of water from the abdomen, but without any special procedures. Just inserting a tube into the abdomen, sometimes bladder and clearing fluid from the area in cases of fluid retention. This is done not only due to renal failure, but also for any diseases resulting in fluid retention.
Continuous Ambulatory Peritoneal Dialysis
In this procedure, a small access (hole) is made in the abdomen and a catheter is inserted. Then, one to two litres of dialysis fluid (Dialysate) is infused into the abdomen and done four to five times a day. In this procedure, there is no diet restriction and can lead a normal lifestyle. This procedure is so named because; it is continuously done and can do any work while in Dialysis.
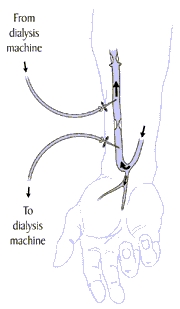
HaemoDialysis
Blood flows opposite to the dialysate and substances are exchanged down a concentration gradient across a semi permeable membrane, between the two compartments.
How HD Works
In haemodialysis, blood is allowed to flow, a few ounces at a time,
through a machine with a special filter that removes wastes and extra fluids.
The clean blood is then returned to the body. Removing the harmful wastes
and extra salt and fluids helps control blood pressure and keep the proper
balance of chemicals like potassium and sodium in the body.
This is because, FCs, if allowed to stay a long time in the body may produce infections, and as the kidney is to be placed near the area of catheter, any infection in the catheter produces infection in the kidney. But, if catheter is inserted in the neck, there is less infection and can be allowed to stay a little longer than FCs.
As I said before, dialysis in catheters is not so effective, because, as a single tube (catheter) is inserted, the same blood will be circulating in the area. Normally, the mechanism of AVF is, joining an artery and a vein. This is to have an access to the artery as veins are easily accessible and arteries are deep in the body. Once, AVF is done, both the pure and impure blood mix and then, pure blood starts flowing in the vein which now acts as an artery. As artery lies deep in the body, there is no access to it like the vein. So AVF is done. The flowing of blood from artery to vein produces a deep vibrating sound in the area of Fistula. It is called a Palpable Thrill, which means, can touch and feel the thrill in the area and also can be identified that it is still working. If it is heard, it sounds like, a train going over a river. If dialysis is done in a Fistula, then the circulation of blood is two way; coming from body to Dialysis Machine and from Dialysis Machine to body. So, 100% is done, if dialysis is in AVF rather than in catheters. Once, surgery is done, the fistula usually stops. But for me, even after months, it is still working.
The other type of vascular access is called Looped Graft where both
the artery and vein are joined together by a graft.
Functions of Dialysis Machine
This machine has three main jobs:
1. Pump blood and monitor flow for safety.
2. Clean wastes from blood.
3. Monitor the Blood Pressure and the Rate of Fluid Removal from body.
The dialyzer is a large canister containing thousands of small fibers
through which blood is passed. Dialysis solution, the cleansing fluid,
is pumped around these fibers. The fibers allow wastes and extra fluids
to pass from the blood into the solution, which carries them away. The
dialyzer is sometimes called an Artificial Kidney.
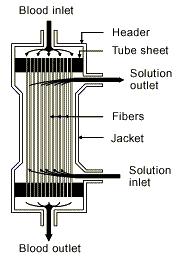
Dialysis solution, also known as dialysate, is the fluid in the
dialyzer that helps remove wastes and extra fluid from the blood. It contains
chemicals that make it act like a sponge.
Needles
There are two types of procedures for the insertion of needles. The first is called the "ladder" strategy for needle placement in which the entire length of the access is done session by session so that one area alone is not weakened with a group of needle sticks. An alternative approach is the "buttonhole" strategy in which the needle is inserted precisely into the same hole made by the previous needle stick.
Anemia and Erythropoietin (EPO)
Anemia is a condition in which the volume of red blood cells is low.
Red blood cells carry oxygen to cells throughout the body. Without oxygen,
cells can't use the energy from food, so someone with anemia may tire easily
and look pale. Anemia can also contribute to heart problems.
Anemia is common in people with kidney disease because the kidneys
produce the hormone erythropoietin, or EPO, which stimulates the bone marrow
to produce red blood cells. Diseased kidneys often don't make enough EPO,
and so the bone marrow makes fewer red blood cells.
Diet
Items to be avoided in diet apart from low intake of fluids are,
1. Potassium - This can be controlled by peeling and soaking the vegetables
in boiling water before cooking, especially potatoes. Some foods rich in
Potassium are oranges, bananas, tomatoes, potatoes, and dried fruits.
2. Phosphorus - Foods like milk and cheese, dried beans, peas, colas,
nuts, and peanut butter are high in phosphorus and should be avoided.
3. Salt (Sodium Chloride) - Of course, high blood pressure and ultimately
more work to the heart.
4. Protein - High quality proteins which come from meat, fish, poultry,
eggs etc can be consumed, but in limited amounts.
Also, this diet is not same for all the patients. As I was not having
previous history of BP and Diabetes, my diet restriction is far less than
patients with some other complications.
The normal weight removal in Dialysis
In all hospitals where dialysis is done, first, they take weight, before
dialysis. When they did this in Guest Hospital, I was not aware of it and
do not why they are recording weight, neither, there would be difference
in pre and post weight of dialysis.
I do not know this weight removal procedure until the mid-dialysis
period in CMC. What they did is, first they take weight before going to
dialysis. For the first HD, they approximately took 2 kilos. Then when
they see if there is no complication then the next time, again they take
weight before going to HD and, subtract the weight from the post-dialysis
weight, which they took during the previous dialysis. For example, if the
pre-dialysis weight is 54kg and post-dialysis weight is 51kg then they
remove 3kg. The next day, if pre weight is 55kg then they remove 4kg. This
3kg and 4kg are called weight loss.
When HD was started in AVF, I began to get many complications like cramps, low BP, etc. During one dialysis, my weight loss is less than 2kg. I went to dialysis and came normally. After this, I came to know that if weight loss is less, then there are no/fewer complications. On that day there was no cramps or other complications for me. This is because, my diet should be much controlled and minimum so that I would not put weight. Also if there is no urine output, the water should be completely restricted as far as possible. In 2 days I would gain a maximum of 4 kilos. But normally no one can be like that, trying to reduce weight because, when in dialysis, there will be increased appetite, and also the psychological feeling that nothing should be taken, increases appetite.
I totally had 17 dialyses, and from that day onwards, except the 16th one, I never got any complications during HD. But I have learnt it only during my last few dialyses.
My Experiences in HD
Though I was anxious about dialysis, I was still happy because I thought
it would be like my previous dialysis without any post-consequences, and
never knew what would generally happen after dialysis, not always, but
very severely.
Since I was getting cramps for a very long time, it was not unusual
for me to get during dialysis and also in chest and abdominal muscles.
If anyone would have seen the movie The Mummy or The Mummy Returns
and noticed that when a scarab (a large black beetle) enters a persons
body, the area where the beetle is in his body would be so bulged, nearly
upto 3 inches in diameter. The same thing happened to me when I got cramps
and the muscles in my chest and stomach would be bulged and rock hard.
My first dialysis was on 5th December 2003 in CMC started at 5:00PM
and was over at 10:00PM. As told you before, the next day I had dizziness
and nausea. Normally I had 4 hours dialysis but one day I had 5 hrs. It
was so boring during this dialysis period. Cannot do any work except lying
in the bed and seeing everyone. Atleast could talk with some people there.
Mostly, people come from East India, so they speak Bengali, I could understand
but cannot speak with them. Then, mostly there are Nepali and Bhutan people.
Before the date of my surgery there were 2 men who were operated earlier.
But I could not see them during dialysis.
As there was less production of Red Blood Corpuscles in the body, during my 5th dialysis they gave me Haemoglobin injection of Rupees 1000/-, as there is a possibility of anaemia. Totally they gave me 11 Injections.
Right from my 6th dialysis, my urine output slowly reduced and at one stage, totally stopped. This is because; they normally stop the function of kidney during dialysis.
The patients can eat anything at the time of dialysis provided they eat / drink, whatever, in the first hour of dialysis.
Dialysis in Femoral Catheter (FC)
As told you before, six times dialysis was done in FC. From 7th onwards dialysis was done in AVF. During the times when Dialysis was done in FC, I would go happily for dialysis, show my catheter and then they do dialysis.
Also, when they knew that I came all the way from Chennai to Vellore, and there are blood clots all over the area of FC, the technicians told me that if there is no blood flow, then, I must have another catheter put in the neck.
As the tube was inside my body, the tubes from dialysis machine are directly connected to my FC. So there was no pain for any reason. Every time before they are starting dialysis, they thoroughly clean the area with antibiotic. So, when they are cleaning the area, there was terrible pain. Even though they are so cautious in handling the FC, still there was pain.
Finally, they inserted both the tubes into FC and connected to the Dialysis machine. Thank God! The blood flow was normal and there was no need for another catheter in the neck.
I wanted to see the thickness of tube (FC), it was 1 cm in thickness but I could not see the length as only a very small portion was outside my body. Finally the dialysis was over that night and subsequently all the following dialysis are done in FC till the Fistula was ready for HD, although with some complications.
The major complications, which generally occur to almost all the patients, are Cramps and Low BP. As already explained before, the reason for Cramps is low calcium and low water in the body and Low BP is low amount of salt in the body. The reason for all these is, naturally, everything removed in Dialysis. Atleast, the complications for dialysis done in FC are far less than done in AVF.
Then, as my Fistula was working so fine, FC was removed on 19th of December and dialysis was immediately started in AVF on 20th of December.
When they removed the catheter from my body, I could finally see its length. It was nearly 7 inches (the tube alone) exclusive of the two small tubes, which are to be connected for dialysis and only half-an-inch, was visible in my body previously. The diameter of tube is nearly 9mm.
Dialysis in Atrio Venous Fistula (AVF)
Finally, dialysis was started effectively in AVF. I was my 7th dialysis. Till 6th, dialysis was done in FC.
I saw many patients where dialysis was done to them in AVF, when I was in FC and could see that they absolutely cannot bear the pain of needle insertion in the AVF site. The technicians normally give local anaesthesia prior to the needle insertion, but still the patients cannot bear pain. On seeing this, I was frightened. When, dialysis was first started in AVF for me, a technician, who knows everything very well regarding dialysis, came and prepared my AVF site. Then to avoid / minimize pain, he first told me to concentrate on some other things other than this needle insertion and began to ask about family, myself and everything. He would be going on ask me, but I would say just a few words. I tried to concentrate a lot, on things other than this, so turned my head to one side and do not want to look it. Normally, a needle insertion would be like a pinprick, but when this needle was inserted, I felt nothing, even no pinprick. Thanks to him. He is the one who first started dialysis to me in AVF and first took blood test during my Follow-up Visits. Then on other consecutive dialyses, the needle insertion was normal and I was accustomed to it. Later, I came to know that everything regarding this depended on the experience of the technicians who come to do dialysis. Also, my hand was over a sterilized towel and the entire needles, gauze piece and everything was sterilized. This is to prevent infection in AVF.
The reason for pain, for the other patients is that, the length of needle is one and a half inch and almost an inch is inserted into the skin. The diameter of needle is nearly 2mm. So only the patients felt pain. Also, after an hour, when the effect of anaesthesia was gone, again there was severe pain in the area of insertion of needles.
Cramps and low BP starts during the last hour of dialysis. This is because; the stuffs are removed very effectively only during the last hour. If cramps occur when we are normal, then we can stand or walk or do anything to minimize it. But if comes during dialysis, it is much horrible. As this is HD, we cannot normally move or get down from bed to minimize cramps. If the cramps are so severe, heavy sweating occurs and BP reduces to a considerably low level. This happens almost every time to me during dialysis.
When cramps come during dialysis, the technicians massage the areas where there were cramps and somehow try to reduce it. If its very severe, then they ask the doctor what to do? and inject saline. Even though its a waste, as the only need for dialysis is removal of water, but they have no option to do. Even for low BP, same thing, and injecting saline till slight recovery and the patient is asked to drink water, as these two things are mainly due to low water in the body. But normally during severe cramps, when we try to drink water, we cannot. It is because the water enters nasal passage rather than mouth.
One day, I came out finishing dialysis with very severe cramps. My mother was talking with a doctor about the next tests she has to take for transplantation. I do not want to disturb her, and want to walk to relieve cramps. So went away and came through the other way to the same place, but my mother was gone. I still had cramps but slightly relieved. When she was not there, I decided to go out of the hospital alone to go home. When I was coming, from the very low level, I could clearly feel what was happening to me. First, slight shivering, then tremors, then tremors increased and head began to pain and started to spin. As the dialysis room is in the first floor, I was walking in the corridor and while all these were happening, I somehow wanted to go and find my mother before I totally faint. Then, after head spinning, tremors still increased and I just stood at a place in the corridor itself and do not want to move. Also, my thinking at that time was I have to go, so I do not know what to do. I just stood there for a couple of minutes and while I was standing, still my head spinning and cannot see anything near me, as everything was blurred. At that time, I had low BP that I almost fainted and that too without anyone (my mother or father) near me in the hospital. Then after some time, I started to recover a little bit and went to my mother as soon as possible.
Even after we went home, its not over yet. Normally, during dialysis, we buy food from hotels for lunch. That day, my mother told she would prepare food. But both of us were in terrible appetite and also, still, I was slightly dizzy. We went home. Then, she cooked potato. Again I started to get cramps, but now in a new place. In my neck! When I tried to eat food, which is my favorite dish, if I open my mouth, I cannot close it, or if close my mouth, cannot able to open it. My mother was so frightened and felt so pathetic at me. At last, with much difficulty, I ate lunch that day.
I normally go walking everyday evening to minimize stress. If there was much cramps and low BP that day, I would go only a little distance, but if there is nothing, then, I would go upto a kilometer and would be enjoying my time while walking as I like walking a lot.
These were my experiences during Dialysis and I like the days of my
Dialysis very much, than my surgery or even post transplant.